Hidden component for CSS inclusion
healthcare is so cooked
thesis
healthcare costs are so high, and processes are so inefficient, largely due to archaic tooling unable to handle a high influx of unstructured data.
the problem
in the US alone, healthcare is one of the biggest industries, contributing about 20% to the overall GDP, roughly $5T.
with that, administrative costs make up roughly 20-25% of this, so about $1T. let me say that one more time: one TRILLION dollars is spent on annoying paperwork instead of physicians dedicating their time to treating their patients with the best possible care.
specifically, physicians spend anywhere from 25-50% of their time on admin work. yes, these people went through a tough several years of medical school to spend half of their time noting things down.
additionally, nearly 50% of patients report at least one symptom of burnout. this is alarming because it is linked to physician turnover, and reduced clinical hours; this is especially troubling amid physician shortages. to distill it, this ultimately impacts your (the patient's) care quality.
what does admin work actually mean
the word "admin work" is tossed around frequently, but what does it actually look like? these are some of the most painful things i saw when shadowing multiple clinics in ontario.
documentation: the physician would write SOAP-format notes for every encounter, whether by phone or an in-person visit. this is a very tedious process to have to constantly flip between being "the kind, empathetic doctor" who is engaged in discussion, to the person who needs to jot information down before they are lost.
paperwork: on average, each patient generates between 0.5-2 documents that need to be filled out. these can come in the form of specialist referrals, lab requisitions, insurance and disability forms, and sick forms, just to name a few of the common ones.
communication: there is a lot of back and forth between clinics and other parties like labs, specialists, and pharmacies for clarification questions and overall coordination. additionally, phoning patients to relay results, schedule follow-ups, or cover any clarifying questions can take up a lot of time in the day.
a doctor i was working with once asked if i watched the show The Bear. he explained that while a single task, like filling out a lab requisition, doesn’t take much time on its own, but the sheer volume of forms he completes each day becomes draining. he referenced the show’s slogan, “every second counts”, noting that the cumulative time lost adds up over the day, compounds over the year, and ultimately reduces the quality of patient care.
tool stack
the root of the problems is the tooling. the primary tool physicians use is the electronic medical record (EMR). these tools are OLD, take a look at the state of the art EMR in canada owned by Telus Health called PS Suite:
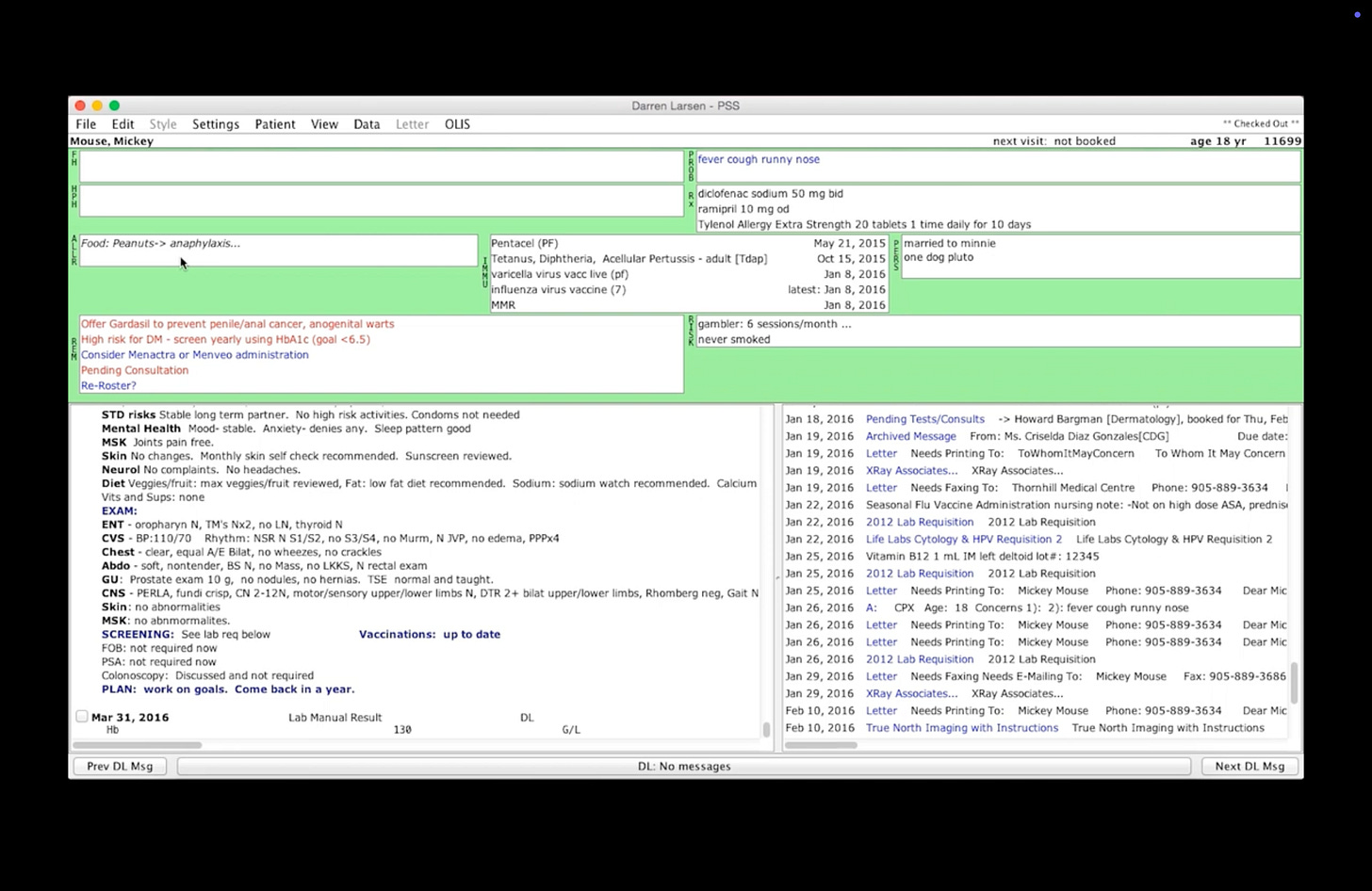
state-of-the-art my foot. this is trash.
the problem with today's EMRs (aside from how much of an eyesore they are) is that they are not made to handle the messy data involved in healthcare. almost all of the data inflows are through faxed forms, emails, and phone calls: unstructured data.
the problem is that EMRs don't actually do much with the data that comes in. the EMR was made during the initial era of the software wave, when we were just trying to digitize everything. yes, it is a "digital" product, but it is merely a "digital analog" product. it is basically a dropbox, where you can scan documents and you have somewhere to store and access them - nothing is actually done with the data. as a matter of fact, 97% of data generated by the healthcare sector goes unused.
rather than a DropBox, we need something like QuickBooks. a product that can take in uploaded documents, and actually extracts data, categorizes expenses, flags duplicates, generates reports, etc.
the opportunity
what EMRs treat as a liability (messy, unstructured data), is actually an asset in the AI/LLM era. we now have the tools available to unlock insights with the 97% of the data that remains unused.
not only can we make more automated processes for these backend admin tasks, the ability to unlock generative insights now becomes possible.
the ultimate end state is an AI-native EMR. we don't need another digital filing cabinet, but a system that leverages every piece of incoming data.
what's next
initially, i sought to build an "AI-native" EMR, and quickly realized that this isn't something that can just be done right away - very naive of me to assume that i found "the first 10-person, $100B company" idea.
i will talk more about the barriers that i faced and why i am pivoting away from this idea in a future post.